The 5,300-year-old Tyrolean Iceman, whose body was found poking out of a glacier in the Italian Alps in 1991, incorporated hides from at least five domesticated and wild animal species into his apparel, a new genetic study finds. Comparing mitochondrial DNA extracted from nine ancient leather fragments with DNA of living animals revealed the makeup of Ötzi’s clothes and a key accessory, says a team led by paleogeneticist Niall O’Sullivan. Mitochondrial DNA typically gets passed from mothers to their offspring. Little is known about what people wore during Ötzi’s time. The findings provide a glimpse into how ancient European populations exploited domesticated animals to make clothes and other items.
Ötzi’s coat consisted of hides from at least three goats and one sheep, the scientists report August 18 in Scientific Reports. This garment may have been periodically patched with leather from whatever animals were available, the team suggests.
Goats also provided skin for the Iceman’s leggings, the new analysis indicates.
A sheepskin loincloth and a shoelace derived from European cattle round out Ötzi’s attire made from domesticated animals.
As for wild animals, Ötzi wore a brown-bear cap and toted a quiver made from roe deer. It’s impossible to know if the ancient man attached any special meaning to brown bears, “but he may have been an opportunistic hunter or a scavenger,” says O’Sullivan, of University College Dublin and EURAC Research in Bolzano, Italy. A 2012 analysis of proteins from fur samples taken from Ötzi’s clothing identified sheep and a goatlike animal called a chamois as sources for the Iceman’s coat. A team led by biochemist Klaus Hollemeyer of Saarland University in Saarbrücken, Germany, also pegged goats and dogs or wolves as sources of skin for Ötzi’s leggings.
Disparities between Hollemeyer’s and O’Sullivan’s studies may stem from the two groups having sampled different parts of patchwork garments. In addition, the new report used advanced techniques for extracting and analyzing ancient DNA. That enabled O’Sullivan’s team to retrieve six complete mitochondrial genomes from Ötzi’s leather belongings.
O’Sullivan’s investigation “opens a new field of potential identification procedures for mammalian species in ancient leathers and furs,” Hollemeyer says.
A roughly 4,200-year-old legging found in the Swiss Alps in 2004 also features goat hide. Mitochondrial DNA extracted from that garment came from an ancient line of European goats that has largely been replaced by a genetically distinct goat population, a team led by archaeologist Angela Schlumbaum of the University of Basel in Switzerland reported in 2010.
The Swiss legging was found with pieces of bows and arrows, woolen clothes and many other artifacts where an ice patch in a mountain pass had partly melted. No human bodies have been found there.
“Possibly, goat leather was most comfortable” as legging material, says University of Bern archaeologist Albert Hafner, a coauthor of the Swiss legging study. “Modern leather trousers often use goat as well.”
Scientists usually shy away from using the word miracle — unless they’re talking about the gene-editing tool called CRISPR/Cas9. “You can do anything with CRISPR,” some say. Others just call it amazing.
CRISPR can quickly and efficiently manipulate virtually any gene in any plant or animal. In the four years since CRISPR has been around, researchers have used it to fix genetic diseases in animals, combat viruses, sterilize mosquitoes and prepare pig organs for human transplants. Most experts think that’s just the beginning. CRISPR’s powerful possibilities — even the controversial notions of creating “designer babies” and eradicating entire species — are stunning and sometimes frightening.
So far CRISPR’s biggest impact has been felt in basic biology labs around the world. The inexpensive, easy-to-use gene editor has made it possible for researchers to delve into fundamental mysteries of life in ways that had been difficult or impossible. Developmental biologist Robert Reed likens CRISPR to a computer mouse. “You can just point it at a place in the genome and you can do anything you want at that spot.”
Anything, that is, as long as it involves cutting DNA. CRISPR/Cas9 in its original incarnation is a homing device (the CRISPR part) that guides molecular scissors (the Cas9 enzyme) to a target section of DNA. Together, they work as a genetic-engineering cruise missile that disables or repairs a gene, or inserts something new where it cuts.
Even with all the genetic feats the CRISPR/Cas9 system can do, “there were shortcomings. There were things we wanted to do better,” says MIT molecular biologist Feng Zhang, one of the first scientists to wield the molecular scissors. From his earliest report in 2013 of using CRISPR/Cas9 to cut genes in human and mouse cells, Zhang has described ways to make the system work more precisely and efficiently.
He isn’t alone. A flurry of papers in the last three years have detailed improvements to the editor. Going even further, a bevy of scientists, including Zhang, have dreamed up ways to make CRISPR do a toolbox’s worth of jobs.
Turning CRISPR into a multitasker often starts with dulling the cutting-edge technology’s cutting edge. In many of its new adaptations, the “dead” Cas9 scissors can’t snip DNA. Broken scissors may sound useless, but scientists have upcycled them into chromosome painters, typo-correctors, gene activity stimulators and inhibitors and general genome tinkerers.
“The original Cas9 is like a Swiss army knife with only one application: It’s a knife,” says Gene Yeo, an RNA biologist at the University of California, San Diego. But Yeo and other researchers have bolted other proteins and chemicals to the dulled blades and transformed the knife into a multifunctional tool.
Zhang and colleagues are also exploring trading the Cas9 part of the system for other enzymes that might expand the types of manipulations scientists can perform on DNA and other molecules. With the expanded toolbox, researchers may have the power to pry open secrets of cancer and other diseases and answer new questions about biology. Many enzymes can cut DNA; the first were discovered in the 1970s and helped to launch the whole field of genetic engineering. What makes CRISPR/Cas9 special is its precision. Scientists can make surgical slices in one selected spot, as opposed to the more scattershot approach of early tools. A few recent gene-editing technologies, such as zinc finger nucleases and TALENs, could also lock on to a single target. But those gene editors are hard to redirect. A scientist who wants to snip a new spot in the genome has to build a new editor. That’s like having to assemble a unique guided missile for every possible target on a map. With CRISPR/Cas9, that’s not necessary.
The secret to CRISPR’s flexibility is its guidance system. A short piece of RNA shepherds the Cas9 cutting enzyme to its DNA target. The “guide RNA” can home in on any place a researcher selects by chemically pairing with DNA’s information-containing building blocks, or bases (denoted by the letters A, T, C and G). Making a new guide RNA is easy; researchers often simply order one online by typing in the desired sequence of bases.
That guidance system is taking genetic engineers to places they’ve never been. “With CRISPR, literally overnight what had been the biggest frustration of my career turned into an undergraduate side project,” says Reed, of Cornell University. “It was incredible.” Reed studies how patterns are painted on butterfly and moth wings. Color patterning is one of the fundamental questions evolutionary and developmental biologists have been trying to answer for decades. In 1994, Sean B. Carroll and colleagues discovered that a gene called Distal-less is turned on in butterfly wings in places where eyespots later form. The gene appeared to be needed for eyespot formation, but the evidence was only circumstantial. That’s where researchers have been stuck for 20 years, Reed says. They had no way to manipulate genes in butterfly wings to get more direct proof of the role of different genes in painting wing patterns.
With CRISPR/Cas9, Reed and Cornell colleague Linlin Zhang cut and disabled the Distal-less gene at an early stage of wing development and got an unexpected result: Rather than cause eyespots, Distal-less limits them. When CRISPR/Cas9 knocks out Distal-less, more and bigger eyespots appear, the researchers reported in June in Nature Communications. Reed and colleagues have snipped genes in not just one, but six different butterfly species using CRISPR, he says.
CRISPR cuts genes very well, maybe too well, says neuroscientist Marc Tessier-Lavigne of Rockefeller University in New York City. “The Cas9 enzyme is just so prolific. It cuts and recuts and recuts,” he says. That constant snipping can result in unwanted mutations in genes that researchers are editing or in genes that they never intended to touch. Tessier-Lavigne and colleagues figured out how to tame the overeager enzyme and keep it from julienning the genes of human stem cells grown in lab dishes. With better control, the researchers could make one or two mutations in two genes involved in early-onset Alzheimer’s disease, they reported in the May 5 Nature. Growing the mutated stem cells into brain cells showed that increasing the number of mutated copies of the genes also boosts production of the amyloid-beta peptide that forms plaques in Alzheimer’s-afflicted brains. The technology could make stem cells better mimics of human diseases. While Tessier-Lavigne and others are working to improve the CRISPR/Cas9 system, building better guide RNAs and increasing the specificity of its cuts, some researchers are turning away from snippy Cas9 altogether.
Nuanced edits Cas9 isn’t entirely to blame for the mess created when it causes a double-stranded break by slicing through both rails of the DNA ladder. “The cell’s response to double-stranded breaks is the source of a lot of problems,” says David Liu, a chemical biologist at Harvard University. A cell’s go-to method for fixing a DNA breach is to glue the cut ends back together. But often a few bases are missing or bits get stuck where they don’t belong. The result is more genome “vandalism than editing,” Liu says, quoting Harvard colleague George Church.
Liu wanted a gene editor that wouldn’t cause any destructive breaches: One that could A) go to a specific site in a gene and B) change a particular DNA base there, all without cutting DNA. The tool didn’t exist, but in Cas9, Liu and colleagues saw the makings of one, if they could tweak it just a bit.
They started by dulling Cas9’s cutting edge, effectively killing the enzyme. The “dead” Cas9 could still grip the guide RNA and ride it to its destination, but it couldn’t slice through DNA’s double strands. Liu and colleagues then attached a hitchhiking enzyme, whose job is to initiate a series of steps to change the DNA base C into a T, or a G to an A. The researchers had to tinker with the system in other ways to get the change to stick. Once they worked out the kinks, they could make permanent single base-pair changes in 15 to 75 percent of the DNA they targeted without introducing insertions and deletions the way traditional CRISPR editing often does. Liu and collaborators reported the accomplishment in Nature in May. A similar base editor, reported in Science in August by researchers in Japan, may be useful for editing DNA in bacteria and other organisms that can’t tolerate having their DNA cut.
There are 12 possible combinations of DNA base swaps. The hitchhiking enzyme that Liu used, cytidine deaminase, can make two of the swaps. Liu and others are working to fuse enzymes to Cas9 that can do the 10 others. Other enzyme hitchhikers may make it possible to edit single DNA bases at will, Liu says. Such a base editor could be used to fix single mutations that cause genetic diseases such as cystic fibrosis or muscular dystrophy. It might even correct the mutations that lead to inherited breast cancer.
Rewriting the score Dead Cas9 is already helping researchers tinker with DNA in ways they couldn’t before. Variations on the dull blade may help scientists solve one of the great mysteries of biology: How does the same set of 20,000 genes give rise to so many different types of cells in the body?
The genome is like a piano, says Jonathan Weissman, a biochemist at the University of California, San Francisco. “You can play a huge variety of different music with only 88 keys by how hard you hit the keys, what keys you mix up and the timing.” By dialing down or turning up the activity of combinations of genes at precise times during development, cells are coaxed into becoming hundreds of different types of body cells.
For the last 20 years, researchers have been learning more about that process by watching when certain genes turn on and off in different cells. Gene activity is controlled by a dizzying variety of proteins known as transcription factors. When and where a transcription factor acts is at least partly determined by chemical tags on DNA and the histone proteins that package it. Those tags are known collectively as epigenetic marks. They work something like the musical score for an orchestra, telling the transcription factor “musicians” which notes to hit and how loudly or softly to play. So far, scientists have only been able to listen to the music. With dead Cas9, researchers can create molecules that will change epigenetic notes at any place in the score, Weissman says, allowing researchers to arrange their own music.
Epigenetic marks are alleged to be involved in addiction, cancer, mental illness, obesity, diabetes and heart disease. Scientists haven’t been able to prove that epigenetic marks are really behind these and other ailments, because they could never go into a cell and change just one mark on one gene to see if it really produced a sour note.
One such epigenetic mark, the attachment of a chemical called an acetyl group to a particular amino acid in a histone protein, is often associated with active genes. But no one could say for sure that the mark was responsible for making those genes active. Charles Gersbach of Duke University and colleagues reported last year in Nature Biotechnology that they had fused dead Cas9 to an enzyme that could make that epigenetic mark. When the researchers placed the epigenetic mark on certain genes, activity of those genes shot up, evidence that the mark really does boost gene activity. With such CRISPR epigenetic editors in hand, researchers may eventually be able to correct errant marks to restore harmony and health.
Weissman’s lab group was one of the first to turn dead Cas9 into a conductor of gene activity. Parking dead Cas9 on a gene is enough to nudge down the volume of some genes’ activity by blocking the proteins that copy DNA into RNA, the researchers found. Fusing a protein that silences genes to dead Cas9 led to even better noise-dampening of targeted genes. The researchers reported in Cell in 2014 that they could reduce gene activity by 90 to 99 percent for some genes using the silencer (which Weissman and colleagues call CRISPRi, for interference). A similar tool, created by fusing proteins that turn on, or activate, genes to dead Cas9 (called CRISPRa, for activator) lets researchers crank up the volume of activity from certain genes. In a separate study, published in July in the Proceedings of the National Academy of Sciences, Weissman and colleagues used their activation scheme to find new genes that make cancer cells resistant to chemotherapy drugs.
RNA revolution New, refitted Cas9s won’t just make manipulating DNA easier. They also could revolutionize RNA biology. There are already multiple molecular tools for grabbing and cutting RNA, Yeo says. So for his purposes, scissors weren’t necessary or even desirable. The homing ability of CRISPR/Cas9 is what Yeo found appealing.
He started simple, by using a tweaked CRISPR/Cas9 to tag RNAs to see where they go in the cell. Luckily, in 2014, Jennifer Doudna at the University of California, Berkeley — one of the researchers who in 2012 introduced CRISPR/Cas9 — and colleagues reported that Cas9 could latch on to messenger RNA molecules, or mRNAs (copies of the protein-building instructions contained in DNA). In a study published in April in Cell, Doudna, Yeo and colleagues strapped fluorescent proteins to the back of a dead Cas9 and pointed it toward mRNAs from various genes. With the glowing Cas9, the researchers tracked mRNAs produced from several different genes in living cells. (Previous methods for pinpointing RNA’s location in a cell killed the cell.) In May, Zhang of MIT and colleagues described a two-color RNA-tracking system in Scientific Reports. Yet another group of researchers described a CRISPR rainbow for giving DNA a multicolored glow, also in living cells. That glow allowed the team to pinpoint the locations of up to six genes and see how the three-dimensional structure of chromosomes in the nucleus changes over time, the researchers reported in the May Nature Biotechnology. A team from UC San Francisco reported in January in Nucleic Acids Research that it had tracked multiple genes using combinations of two color tags.
But Yeo wants to do more than watch RNA move around. He envisions bolting a variety of different proteins to Cas9 to manipulate and study the many steps an mRNA goes through between being copied from DNA and having its instructions read to make a protein. Learning more about that multistep process and what other RNAs do in a cell could help researchers understand what goes wrong in some diseases, and maybe learn how to fix the problems.
Zhang wants to improve Cas9, but he would also like other versatile tools. He and colleagues are looking for such tools in bacteria.
CRISPR/Cas9 was first discovered in bacteria as a rudimentary immune system for fighting off viruses (SN: 12/12/15, p. 16). It zeroes in on and then shreds the viral DNA. Researchers most often use the Cas9 cutting enzyme from Streptococcus pyogenes bacteria.
But almost half of all bacteria have CRISPR immune systems, scientists now know, and many use enzymes other than Cas9. In the bacterium Francisella novicida U112, Zhang and colleagues found a gene-editing enzyme, Cpf1, which does things a little differently than Cas9 does. It has a different “cut here” signal that could make it more suitable than Cas9 for cutting DNA in some cases, the team reported last October in Cell. Cpf1 can also chop one long guide RNA into multiple guides, so researchers may be able to edit several genes at once. And Cpf1 cuts DNA so that one strand of the DNA is slightly longer than the other. That could make it easier to insert new genes into DNA.
Zhang more recently found an enzyme in the bacterium Leptotrichia shahii that could tinker with RNA. The RNA cutting enzyme is called C2c2, he and colleagues reported August 5 in Science. Like Cas9, C2c2 uses a guide RNA to lead the way, but instead of slicing DNA, it chops RNA.
Zhang’s team is exploring other CRISPR/Cas9-style enzymes that could help them “edit or modulate or interact with a genome more efficiently or more effectively,” he says. “Our search is not done yet.”
The explosion of new ways to use CRISPR hasn’t ended. “The field is advancing so rapidly,” says Zhang. “Just looking at how far we have come in the last three and a half years, I think what we’ll see coming in the next few years will just be amazing.”
White, fierce and fluffy, snowy owls are icons of Arctic life. But some of these owls are not cool with polar winters.
Every year, part of the population flies south to North American prairies. Ornithologists thought those birds fled the Arctic in desperation, haggard and hungry. But the prairie owls are doing just fine, researchers report August 31 in The Auk: Ornithological Advances.
Over 18 winters, wild snowy owls caught and banded in Saskatchewan, Canada — one of the species’ southerly destinations — were 73 percent heavier than emaciated owls in rescue shelters. Females were heavier and had more fat than males, and adults were in better condition than youngsters. But regardless of age or sex, most snowy owls that made the journey south were in relatively good health.
That means southern winters may not be such a desperate move after all. Prairies are probably just a normal wintering ground for some of the Arctic snowy owl population, the researchers say. Snowbirds, indeed.
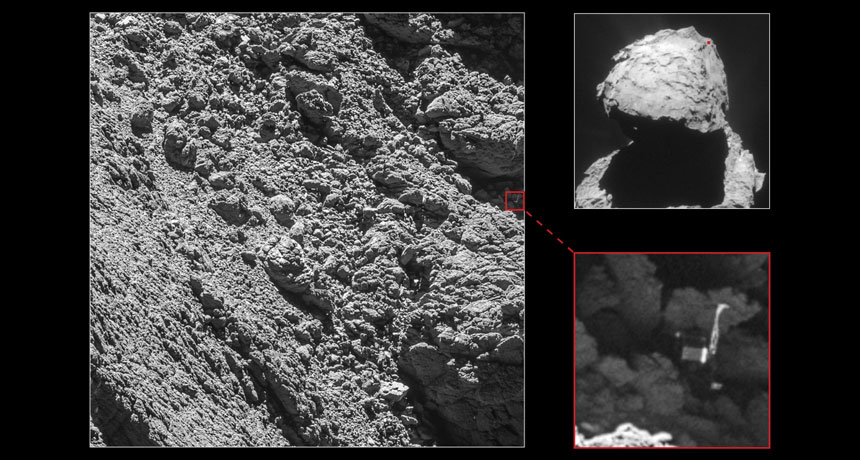
Philae has been found, nestled in a shadowy crevice on comet 67P/Churyumov-Gerasimenko. The comet lander, lost since its tumultuous touchdown on the comet on November 12, 2014, turned up in images taken by the Rosetta orbiter on September 2.
Philae is on its side with one leg sticking out into sunlight. Its cockeyed posture probably made it difficult for Philae to reliably get in touch with Rosetta, explaining why scientists had trouble reestablishing communication. The discovery came about a month before the end of the Rosetta mission; the orbiter was scheduled to land on the comet on September 30and then shut down.
Philae spent just a few days transmitting data from the comet’s surface (SN: 8/22/15, p. 13). It had a rough landing, bouncing twice before stopping. Sitting in the shadow of a cliff, Philae was unable to use solar power to recharge its battery. Rosetta picked up intermittent communication in June and July 2015. Since January, temperatures on the comet have been too chilly for Philae’s electronics; scientists stopped listening for radio signals in July.
Pterosaurs didn’t have to be gargantuan to survive in the Late Cretaceous.
Fragmentary fossils of a roughly 77-million-year-old pterosaur found in British Columbia suggest it had a wingspan of just 1.5 meters, close to that of a bald eagle. The ancient flier is the smallest pterosaur discovered during this time period — by a lot, report paleontologist Elizabeth Martin-Silverstone of the University of Southampton in England and colleagues August 30 in Royal Society Open Science.
Dozens of larger pterosaurs, some with wings spanning more than 10 meters (nearly the length of a school bus), have been unearthed. But until now, scientists had found only two small-scale versions, with wingspans 2.5 to 3 meters long, from the period stretching from 66 million to 100 million years ago.
Some scientists blamed competition with birds for the scarcity of little flying reptiles. Researchers have proposed that, “the only way pterosaurs could survive was by evolving completely crazy massive sizes,” Martin-Silverstone says.
The new find, she says, may mean that, “pterosaurs were doing better than we thought.”
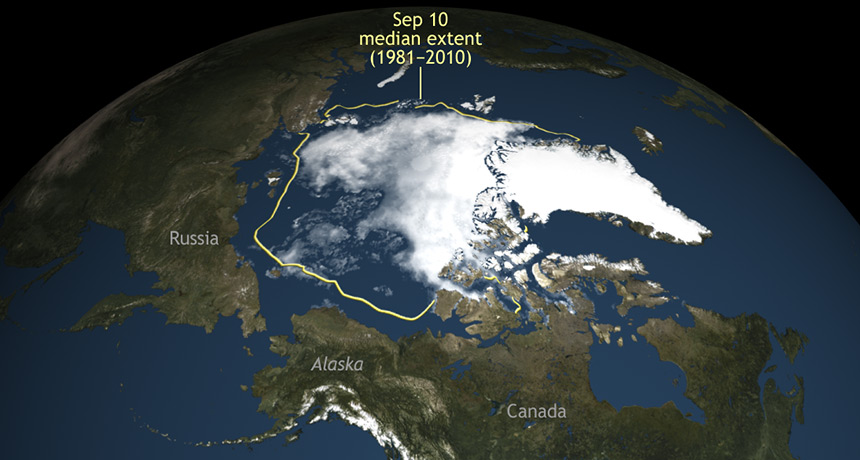
Sea ice around the North Pole has reached its second-lowest low on record, tying with 2007, scientists at NASA and the National Snow and Ice Data Center announced September 15.
Arctic sea ice reached its expected low point for the year on September 10, bottoming out at an area of 4.14 million square kilometers. That’s well below the 1981 through 2010 average of 6.22 million square kilometers, though above the record-lowest extent of 3.39 million square kilometers, set in 2012.
The silver-medal finish came after a summer of relatively cool temperatures, cloudy skies and stormy weather — conditions that typically limit sea ice shrinkage. The lack of ice probably arose from a poor starting position: The melt season began with the smallest maximum sea ice extent on record.
Shrinking sea ice can speed up warming, threaten Arctic species and spread pollution.
Qian Chen, 30 Materials scientist University of Illinois
The SN 10 In a darkened room, bathed in the glow of green light, materials scientist Qian Chen watches gold nanorods dance. They wiggle across a computer screen displaying real-time video from a gigantic microscope — a tall, beige tube about as wide as a telephone pole.
Chen has observed these and other minuscule specks of matter swimming, bumping into one another and sometimes organizing into orderly structures, just like molecules in cells do. By pioneering the design of new biologically inspired materials, she’s exploring what it means to be “alive.” Next, Chen wants to get an up-close and personal view of cellular molecules themselves: the nimble, multitasking proteins that work day and night to keep living organisms running.
At age 30, Chen is already racking up high-profile publications and turning some far-out ideas into reality. Her ultimate goal: To mimic the machinery that living cells have already perfected. To create life, or something like it, out of nonliving materials.
“If you can see it, you can start to understand it,” Chen said when I visited her lab at the University of Illinois at Urbana-Champaign earlier this year. “And if you understand it, you can start to control it.”
Chen didn’t always want to be a scientist. Growing up in China, she imagined one day becoming a writer. In middle school, she wrote an award-winning story about a girl who figures out how to repair the ozone layer. “My idea was to get some material that can be stretched, like the skin of the balloon,” Chen says. Her interest in inventing new and unusual materials took off years later, in the United States. After graduating from college in China in 2007 — Chen was the first in her family to do so — she headed to Illinois to work with materials scientist Steve Granick.
From the start, Chen stood out. “She made hard things look easy,” says Granick, now at the Ulsan National Institute of Science and Technology in South Korea. He recalls one experiment in particular, when Chen performed a feat some scientists thought impossible: She got thousands of tiny beads to form an open and orderly two-dimensional structure — all by themselves.
Chen had been studying colloidal particles, microscopic specks roughly a micrometer in size. People normally think of these particles as a component of paint, not all that interesting.
But Chen had the idea to cover the particles with a kind of sticky coating that acted something like Velcro. When the particles bumped into one another, they stuck together. At first, “It looked like a mess, like a failed experiment,” says Granick. “Most graduate students would have just chalked it up to a mistake and gone home.”
After a day of knocking around in solution, sticking together and tearing apart, the particles finally settled into something stable. The special coating and the way Chen applied it (capping the top and bottom of each particle) led to a “kagome lattice,” something sort of like a honeycomb. Never before had scientists coaxed colloidal particles into such an open, porous framework. Usually, the particles pack together more tightly, like apples stacked on the shelf at a grocery store, Chen says. That work led in 2011 to a publication in Nature: “Directed self-assembly of a colloidal kagome lattice.” A week earlier, Chen and Granick had published a different paper in Science, “Supracolloidal reaction kinetics of Janus spheres,” about particles that self-assemble into a twisting chain, or helix. At the time, Chen was 24.
“Her work is at the leading edge,” says Penn State chemist Christine Keating. “She’s so full of enthusiasm for science, and energy and creative ideas.”
Exactly how such particles might one day be used is still anybody’s guess. Some researchers envision self-assembling materials building smart water filters or adaptable solar panels that change shape in response to the sun. But the full range of possibilities is hard to fathom. Chen is “trying to invent the rules of the game,” Granick says. “She’s laying the groundwork for future technologies.”
Her next big focus will take her field from self-assembly 101 to the master class level, by mimicking how biological molecules behave. But first she has to see them in action.
Into the cell In 2012, Chen traveled west to the University of California, Berkeley to work with National Medal of Science winner Paul Alivisatos on a new microscopy technique.
Scientists today can view the details of proteins and DNA close up under a microscope, but the results are typically still-life images, frozen in time. It’s harder to get action shots of proteins morphing in their natural, fluid world. That view could unveil what roles different protein parts play.
Even a technique that won its developers a Nobel Prize in 2014 (SN: 11/2/14, p. 15) — it relies on fluorescent molecules to illuminate a cell’s moving parts — can’t always reveal the intricacies of proteins, Chen says. They’re just glowing dots under the microscope. Imagine, for example, looking at a dump truck from an airplane window. You can’t see how the truck actually works, how the pistons help lift the bed and the hinges open the tailgate.
“I use this as inspiration,” Chen says, grabbing her laptop and starting up a video that may well be the fantasy of anyone exploring biology’s secret world. The computer animation shows molecules whizzing and whirling deep inside a cell. Gray-green blobs snap together in long chains and proteins haul giant, gelatinous bags along skinny tracks. No one yet has gotten a view as clear as this hypothetical one, but a technique Chen is now helping to develop at Illinois could change that.
It’s called liquid-phase transmission electron microscopy, and it’s a slick twist on an old method. In standard TEM, researchers create subnanometer-scale images by shooting an electron beam through samples placed in a vacuum. But samples have to be solid — still as stone — because liquids would evaporate.
By sandwiching beads of liquid between thin sheets of graphene, though, Chen gets around the problem. It’s like putting droplets of water in a plastic baggie. The liquid doesn’t dry up, so researchers can observe the particles inside jittering around. Chen has used the technique to see gold nanorods assembling tip-to-tip and DNA-linked nanocrystals moving and rotating in 3-D. Now, she may be on the verge of a big advance.
With liquid-phase microscopy, Chen is attempting to see cellular machinery with a clarity no scientist has achieved before. She is cautious about revealing too many details. But if Chen succeeds, she may be on her way to cracking the code that links biological structure to function — figuring out the parts of a protein, the pistons and hinges, that let it do its specific job. Knowing the structural building blocks of life, she says, will help scientists create them — and everything they can do — out of artificial materials.
“We’re not there yet,” Chen says, “but that’s the big dream.”
A baby boy born on April 6 is the first person to be born from a technique used to cure mitochondrial diseases, New Scientist reports.
The child’s mother carries Leigh syndrome, a fatal disease caused by faulty mitochondria. Mitochondria generate most of a cell’s energy and perform other functions that keep cells healthy. Each mitochondria has a circle of DNA containing 37 genes needed for mitochondrial function. A mutation in one of those genes causes Leigh syndrome. The woman herself is healthy, but previously had two children who both died of Leigh syndrome.
John Zhang, a fertility doctor at New Hope Fertility Center in New York City, and colleagues transferred a structure called the spindle with chromosomes attached to it from one of the woman’s eggs into a healthy, empty donor egg. The resulting egg was then fertilized with sperm from the woman’s husband. The procedure was done in Mexico.
The technique, called spindle nuclear transfer, is one of two ways of creating “three-parent babies” to prevent mitochondrial diseases from being passed on. Such three-parent babies inherit most of their DNA from the mother and father, but a small amount from the donor. Other three-parent children who carried mitochondria from their mothers and from a donor were born in the 1990s, but the baby boy is the first to be born using a nuclear transfer technique. Zhang and colleagues will report the successful birth October 19 in Salt Lake City at the American So
Murder was a calculated family affair among Iceland’s early Viking settlers. And the bigger the family, the more bloodthirsty.
Data from three family histories spanning six generations support the idea that disparities in family size have long influenced who killed whom in small-scale societies. These epic written stories, or sagas, record everything from births and marriages to deals and feuds.
Iceland’s Viking killers had on average nearly three times as many biological relatives and in-laws as their victims did, says a team led by evolutionary psychologist Robin Dunbar of the University of Oxford. Prolific killers responsible for five or more murders had the greatest advantage in kin numbers, the scientists report online September 20 in Evolution and Human Behavior. Particularly successful killers chose their victims carefully, knowing that their large families would deter revenge attacks by smaller families of the slain, the researchers contend. Those killings were motivated by land grabs, they suspect. One-time killers tended to have only slightly bigger families than those of their victims; insults or goading possibly prompted those murders. Strikingly, around 18 percent of all men mentioned in the sagas were murdered. Similarly high homicide rates, mainly due to cycles of revenge killing between feuding families, have been reported for some modern hunter-gatherer and village-based societies ( SN Online: 9/27/12 ). Lethal raids by competing groups may go back 10,000 years or more ( SN: 2/20/16, p. 9 Murder rates rise in the absence of central authorities that enforce social order, Dunbar proposes. “The real issue is not that there were so many murders among Icelandic Vikings, but that murders were carefully calculated based on knowing whether one had a sufficient family advantage to take the risk.”
That idea relates to mathematical formulas of fighting strength developed during World War I by British engineer Frederick Lanchester. One of Lanchester’s laws calculates that the fighting advantage of a larger group over a smaller group grows disproportionately as the disparity in the size of war parties increases. That rule also holds for family-size differences in small-scale societies, such as Icelandic Vikings, Dunbar’s group concludes.
Tests of the possibility that greater kin numbers encourage lethal attacks in preindustrial groups, such as the Vikings, are rare, says Oxford evolutionary biologist and political scientist Dominic Johnson, who did not participate in the new study. Johnson has reviewed evidence suggesting that humans, chimps and social hunters such as wolves have evolved ways to monitor group sizes and launch attacks when they can gang up on a few opponents.
Dunbar and his colleagues studied three Icelandic family sagas covering events from around 900 to 1100. Iceland’s first settlers arrived from Scandinavia and northern Europe in the late 800s (SN: 5/14/16, p. 13).
The sagas contained information about events, including feuds and murders, involving 1,020 individuals. For everyone mentioned, the researchers identified a network of biological and in-law relationships.
Under Norse law, a murder entitled a victim’s relatives to compensation, either via a revenge murder or blood money. Icelandic sagas describe the importance of avenging murdered relatives to save face and prevent further attacks, regardless of family size.
In the three sagas, a total of 66 individuals caused 153 deaths; two or more attackers sometimes participated in the same killing. No killers were biologically related to their victims (such as cousins or closer), but one victim was a sister-in-law of her killer.
About two-thirds or more of killers had more biological kin on both sides of their families, and more in-laws, than their victims did.
Six men accounted for about 45 percent of all murders, each killing between five and 19 people. Another 23 individuals killed two to four people. The rest killed once. Frequent killers had many more social relationships, through biological descent and marriage, than their victims did, suggesting that they targeted members of families in vulnerable situations, the researchers say.
Apes understand what others believe to be true. What’s more, they realize that those beliefs can be wrong, researchers say. To make this discovery, researchers devised experiments involving a concealed, gorilla-suited person or a squirreled-away rock that had been moved from their original hiding places — something the apes knew, but a person looking for King Kong or the stone didn’t.
“Apes anticipated that an individual would search for an object where he last saw it, even though the apes knew that the object was no longer there,” says evolutionary anthropologist Christopher Krupenye. If this first-of-its-kind finding holds up, it means that chimpanzees, bonobos and orangutans can understand that others’ actions sometimes reflect mistaken assumptions about reality. Apes’ grasp of others’ false beliefs roughly equals that of human 2-year-olds tested in much the same way, say Krupenye of the Max Planck Institute for Evolutionary Anthropology in Leipzig, Germany, and his colleagues.
Considering their targeted gazes during brief experiments, apes must rapidly assess others’ beliefs about the world in wild and captive communities, the researchers propose in the October 7 Science. Understanding the concept of false beliefs helps wild and captive chimps deceive their comrades, such as hiding food from those who don’t share, Krupenye suggests.
Experiments included 41 apes — 19 chimps, 15 bonobos and seven orangutans. These animals had been born in captivity and lived in open enclosures at research centers in Germany and Japan. Apes watched two short videos designed to grab their attention. In one, a person in a King Kong gorilla suit hides in one of two haystacks while a man watches. After the man leaves through a door, King Kong runs away. Then the man returns and looks for King Kong. In a second video, a man returns for a stone that King Kong stole from him and hid in one of two boxes while the man watched. During the man’s absence, however, King Kong runs off with the stone or, in another version, moves the stone from one box to the other.
A camera equipped with an eye-tracking sensor revealed that, when the man in these videos returned, apes usually looked first at where King Kong or the stone had initially been hidden. They also spent more time looking at those initial locations than at any other spots in the videos. Those behaviors indicate that the apes assumed the man would return to those same spots based on where he had last seen what he was looking for. Of 29 animals that viewed both videos, gazes of 23 indicated that they expected the man in one or both scenarios to hold a false belief, the researchers say. Krupenye’s team shows for the first time that a nonhuman animal can track others’ false beliefs, agrees psychologist Amanda Seed of the University of St. Andrews in Fife, Scotland. But it has yet to be demonstrated that apes, like humans, can act on such knowledge, say by hiding food from others, she adds. It’s also unclear whether, aside from knowing where an observer will look for an item, apes truly know that the object is no longer there, Seed says. Further experiments could see if apes express surprise upon seeing an observer find an item hidden in its original location after it had been moved, she suggests.
An ability to infer what others are thinking, dubbed “theory of mind” by psychologists (SN Online: 3/27/13), likely evolved in ancient ancestors of humans and apes, writes primatologist Frans de Waal of Emory University in Atlanta in the same issue of Science. Those ancestors lived in increasingly complex communities where it paid to predict accurately how others would behave, he proposes.
Yale University psychologist Laurie Santos isn’t so sure apes track false beliefs. Previous research has consistently indicated that no nonhuman animals monitor others’ beliefs, even on tasks similar to those used by Krupenye’s team, Santos says. In the new study, she adds, apes may have realized that an observer was ignorant about an object’s new location but not that he had false expectations about where to find it.
Krupenye disagrees. “The apes specifically anticipated that the actor in the video would search for an object where we humans know the actor falsely believed the object to be,” he says.