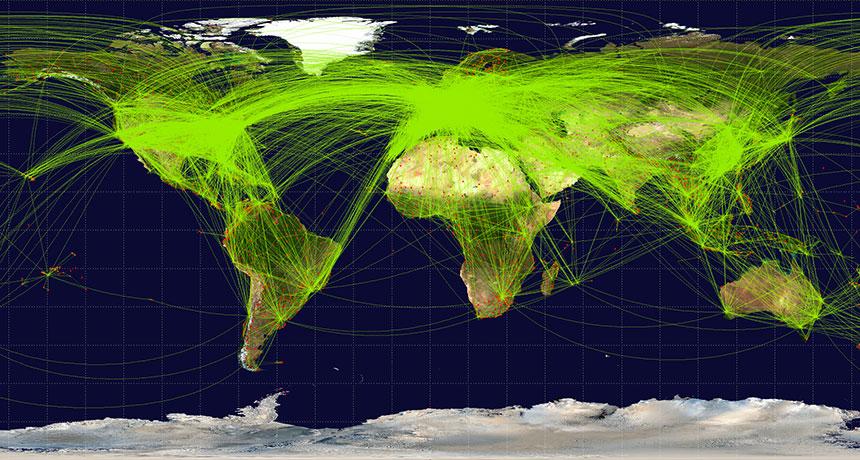
Global tourism contributes about 8 percent of total greenhouse gas emissions to the atmosphere, researchers report May 7 in Nature Climate Change. That carbon footprint is about three times as large as tourism-related emissions estimated by previous studies.
The jump is largely because the new study doesn’t just tally up emissions from the traveling itself, like hopping a flight, going on a road trip or taking a cruise. It also looks at the impact of the goods and services that tourists enjoy, from food to shopping to hotel stays. Who has the biggest carbon footprint? The United States topped the list, as both a top destination for tourists and a source of tourists. Other prosperous nations, such as Canada and Germany, also have a big footprint, and increasingly wealthy nations, such as China and Mexico, are catching up in this amazing race.
Take a look at global tourism by the numbers:
4.5 gigatons The amount of carbon dioxide and other greenhouse gases that came from tourism in 2013.
2.7 percent The share of the global total of emissions that comes just from Canadians and Mexicans traveling to the United States for tourism.
300 kilograms Increase, from 2009 to 2013, in the yearly carbon footprint for each inhabitant of the tiny island nation of the Maldives as a result of international tourism.
$4.7 trillion The amount of money, in U.S. dollars, spent on global tourism in 2013. That’s up from $2.5 trillion in 2009.
3 percent Current annual growth in money spent on global tourism, which translates to tourism-related emissions of 6.5 gigatons of carbon dioxide and other greenhouse gases by 2025.
It’s vacation season — time for swimming pools, hot tubs and water parks. But you might want to think twice before getting wet, says a new report from the U.S. Centers for Disease Control and Prevention.
From 2000 to 2014, public health officials from 46 states and Puerto Rico reported 493 outbreaks associated with treated recreational water, resulting in more than 27,000 illnesses and eight deaths, according to a report in the May 18 Morbidity and Mortality Weekly Report. Hotel pools and hot tubs were the setting for about a third (32 percent) of the outbreaks, followed by public parks (23 percent), club/recreational facilities (14 percent) and water parks (11 percent).
Most of the infections were from three organisms that can survive chlorine and other commonly used disinfectants: Cryptosporidium, a parasite that can cause gastrointestinal problems; Pseudomonas, a bacteria that causes swimmer’s ear; and Legionella, a bacteria that causes a pneumonia-like illness.
So, what to do? The CDC recommends a few steps before diving in: Don’t swallow pool water. Don’t let children with diarrhea in the water. And use test strips to measure levels of pH, bromine and chlorine in the water. The cleaner the water, the safer to swim.
When severe, chronic diarrhea strikes, sometimes the only cure is … more feces. It might seem bizarre, but a transplant of healthy human stool and its bacterial ecosystem can mean freedom from a painful, life-threatening illness.
The transplants — called fecal microbiota transplants, or FMTs — are becoming more and more popular. So popular that the stool bank OpenBiome has supplied more than 30,000 stool samples to clinicians and scientists since 2012. Right now, though, the government isn’t quite sure how to regulate fecal transplants. That uncertainty comes from what seems like a simple question: What is poop? Is it a drug? Is it a bodily tissue? Is it a little of both? Then, is the transplant itself a procedure? That’s a whole other regulatory category.
Out of concern that regulations would cut out desperate patients or send companies running to more profitable enterprises, some FMTs aren’t actually regulated at all. That leads to the potential for unscreened and potentially dangerous fecal samples to flood the market. A group of doctors and scientists from the University of Maryland School of Medicine in Baltimore have tried to cut through the confusion with a three-track policy plan that would help keep poop transplants clean (as clean as fecal matter gets, anyway), while still allowing patients to get transplants when they need them. The scientists also hope to encourage companies to develop potentially lucrative products for future FMTs — including options that are almost feces-free.
A fecal transplant involves taking a mixture of a donor’s poop and saline (sometimes mixed with the help of a kitchen blender) and inserting it into a patient’s large intestine or far down the gut with a nasogastric tube. Companies are working on alternatives to that procedure, such as pills that deliver the same benefits with less of an “ick” factor. Currently, FMTs have the most potential for treating Clostridium difficile infections. C. diff is a bacterium normally found in our guts and feces. But unchecked, it can take over the large intestine. The result is inflammation and chronic severe diarrhea that can last weeks or months. There are more than 450,000 estimated cases in the United States each year, and more than 29,000 deaths. Doctors can prescribe antibiotics to kick the bugs out, but in 20 percent of patients, the infection comes back again. And again.
For those patients, FMTs can be a miracle. They resolve symptoms in 85 percent of patients with recurrent C. diff infections, compared with the roughly 20 to 30 percent success rates of antibiotics.
Unfortunately, FMTs also come with a dose of danger. Feces is a mixture of our undigested waste, the beneficial microbes needed to keep our guts healthy and whatever bacteria, fungi and viruses we’ve picked up in our busy lives. So donors need to be screened for pathogens that might make a sick recipient sicker. And the poop needs to be handled carefully to avoid contamination or infection in the people who handle and receive it.
Gastroenterologist Erik von Rosenvinge of the University of Maryland School of Medicine in Baltimore has performed more than 40 FMTs. “When I first started doing these in 2013, I was having the patients identify a friend or family member, and they would bring in the stool and I would process it myself,” he says. After the first few donations, von Rosenvinge switched to using stool from the OpenBiome stool bank. It saves money and time.
For each donation, the stool bank or hospital will test the feces for pathogens. But who sets the standard to ensure that people getting treated for C. diff are receiving “clean” stool, either from their friends or from a stool bank?
Well, right now, no one.
Poop: Drug or tissue? The first problem is to figure out what an FMT actually is, at least, in terms of how the government should regulate one. Feces is like a drug, in that the microbes in it can change how the body functions. But because of those very microbes, feces is also a living thing that differs from person to person. In fact, in some ways, poop is like biological tissue, in that it comes from the human body.
But then, the FMT itself is something like a procedure — there’s a method involved in getting one. But that procedure is also delivering a drug. Or is it transplanting a tissue? Here we go again.
“The FDA has been reticent to create a new regulatory product category,” says Jacques Ravel, who studies the microbiome and women’s health at the University of Maryland School of Medicine. “They’ve been trying to fit the stool into one of the regulated product categories, and there’s limitations every time you do, there’s pros and cons.”
In 2013, the FDA declared that FMTs counted as a drug (technically a “live biotherapeutic product”) in terms of how they would be regulated, which, von Rosenvinge notes, “means all of us are pharmaceutical factories,” pooping out “drugs” once a day on average.
But FMTs don’t have FDA approval yet, so as a drug, an FMT is considered “investigational.” Giving one to a patient would require an investigational new drug application, or IND. Those are associated with clinical trials, meaning someone who needed an FMT would probably have to get into a clinical trial to get treatment. “At that point [in 2013], I’d only done a handful, and I had to stop because I didn’t have an IND,” von Rosenvinge recalls.
The FDA’s goal was to make sure that FMTs were safe for people. But the requirements meant that most doctors could not give FMTs. At a public workshop about FMTs in 2013, scientists and physicians spoke out against the requirements. In response, the FDA noted that it would practice “enforcement discretion.” That’s government-speak for politely looking the other way while doctors treated C. diff patients outside of clinical trials.
Unfortunately, looking the other way means that FMTs — whether prepared from a donor by a doctor or purchased from a stool bank — are still completely unregulated. As FMTs gain popularity for C. diff, von Rosenvinge notes, that could lead to problems. “You don’t want someone grabbing poop out of the local [port-a-potty] and selling it. That would be horrible,” he says. “If someone’s going to be using stool to put into a human, you want to have assurances that it was properly handled, that the donor was properly screened, that we’re doing everything within reason to minimize risk of causing problems.”
The stool banks themselves aren’t pleased with the arrangement, either. “We’re all operating on a bit of uncertainty,” says Carolyn Edelstein, the executive director of OpenBiome. Right now, OpenBiome screens all of their samples by their own standards, because the government hasn’t given them any. Everyone knows that “looking the other way” could end at any time, a move that the FDA proposed in March 2016. Then, INDs would be required again, and patients could be out of luck.
Balancing regulation and access To patients, access — cheap access — is paramount. “The big challenge at the end of the day is access to treatment, and the fact that FMT is really cheap as its performed right now,” says Ravel. “Right now there’s no true alternative, even those coming down the pipe may be able to cure [C. diff], but they’re not going to be cheap.”
But to doctors, scientists and government, access needs to be balanced with safety. “People are doing this at home, and I think that raises issues about the safety of donations,” notes Diane Hoffman, who studies health law at the University of Maryland. “Do [patients] understand the potential for contamination and disease transmission?”
The right balance might also help promote the development of new drugs for treating C. diff — ones that extract the most useful bacteria, for example, and don’t involve an enema.
To this end, Hoffman, von Rosenvinge, Ravel and colleagues worked with a large working group of scientists, lawyers, industry partners and patient advocates to come up with recommendations for regulating FMTs, which they outlined in December in Science. The result is a slim, three-track system.
Individual FMTs for C. diff done by doctors with donors who are friends or family of the patients would be classified under “practice of medicine.” This is an exception that allows doctors to use their expertise and judgment when treating patients, as long as the treatments they’re using are legally available. No FDA approval or IND required. “We’re trusting the doctor to do what’s in the best interests of the patient,” Hoffman explains.
Stool banks, on the other hand, would be regulated like tissue banks. They’d have to comply with good manufacturing and safety practices and screen and test their donors. The banks would also have to track the patients who receive donations, and submit their long-term data to a national registry. The banks would be free to sell FMT samples, but only to treat C. diff. Any other use that the FMT hasn’t been approved for would still require a clinical trial.
The third track would be for “stool-based products.” These would be pills or delivery systems that offer, say, combinations of microbes, rather than the current practice of basically “polishing a turd,” notes von Rosenvinge. These would be regulated as biological products or drugs.
In practice, this would mean stool banks and stool transplants would be regulated more like cell and tissue banks and transplants. “Stool-based products” on the other hand, would be regulated more like drugs. No matter what, patients would have to be informed of all the risks associated with an FMT. “I think the stand-out, excellent point of this proposed regulatory scheme is that stool banks need to be regulated, and there need to be rigorous data collection of outcomes,” says Kelly Hills, a bioethicist with Rogue Bioethics. “Track everything. The whole enchilada. We have historical precedents [such as in vitro fertilization] where we didn’t track outcomes, and 20 or 40 years down the line we’ve been kicking ourselves. It’d be nice to learn from our mistakes!”
This is especially important because while FMTs have very clear benefits for C. diff in the short term, no one really knows what the long-term effects will be. “We don’t have a lot of [long-term data] right now,” Hills notes. “We know that when you change someone’s gut microbiome you actually change a lot in their life. We have the anecdotal stories of people losing lots of weight, for example, or people’s dietary desires changing.” But the plural of anecdote isn’t data. A registry might help scientists keep track of exactly what transplants people received and their long-term effects.
But “practice of medicine” might give too much leeway to doctors to try FMT for things that they probably shouldn’t, worries Leigh Turner, a bioethicist at the University of Minnesota in Minneapolis. “‘Practice of medicine’ isn’t a curb on advertising or promotional claims,” he notes.
The group behind the policy proposal was careful not to stand in the way of further drug development. That third track was designed with the hope of promoting stool-based products, so that companies might be encouraged to pursue more of them. But if FMTs aren’t broken, why would companies — let alone patients — want to take the risks to fix them? With FMTs freely available, it might be hard to recruit patients to potential clinical trials for new drugs. “If you have a cheap solution that works and you have a patient with C. diff, that patient will not want to enter a trial with a placebo arm,” notes Ravel. After all, what if they got the placebo? They want a cure, not a game of roulette.
The policy brief isn’t policy, and the FDA hasn’t made a final call. But looking the other way isn’t going to cut it in the long term. FMTs are only used for recurrent C. diff infections right now. But scientists are interested in them for many other things. “You can get into weird science fiction areas. Would athletes start doing FMTs to try and improve their Tour de France time? Could you lose weight?” notes Hills. Some of these could be lucrative options for companies. And because FMTs are so easy to perform, people are already making headlines with the do-it-yourself route.
No matter what, a lack of regulation isn’t a long-term strategy. People are going to find other uses for feces, and the FDA will need to be prepared when they do.
Decades ago, pregnant women had to wait about 40 weeks before knowing much about their baby. But swiftly moving technology offers increasingly detailed peeks into the womb.
Beyond generating adorable 3-D ultrasounds of scrunched-up faces, researchers can now analyze a fetus’s full genome from a simple blood draw from mom. But these genome-wide prenatal tests are not ready for prime time, three medical organizations argued in a position paper in the January Prenatal Diagnosis.
The method is undoubtedly powerful. Scanning the entire genome can reveal DNA abnormalities that more limited genetic tests might miss. But scientists don’t know enough about the performance of these tests, or their pitfalls, to recommend routine use, wrote representatives from the International Society for Prenatal Diagnosis, the Perinatal Quality Foundation and the Society for Maternal-Fetal Medicine. How to interpret the information these tests provide is not always obvious. Many genetic quirks have little or no influence on human health, and sifting through a mountain of genetic data to identify the important signals isn’t easy. So far, large studies that could reveal the utility of these tests simply haven’t been done. Ethical and practical issues dog these whole-genome tests, too. Identifying a potentially fatal genetic abnormality can be straightforward. But often, the relationship between genetics and outcomes is less clear. Researchers are still figuring out how specific genetic changes — or more likely, combinations of many genetic changes — relate to genetically influenced disorders such as autism spectrum disorder or to a risk of dementia in the baby’s distant future. How doctors or parents should handle this murkier information is an open question.
And then there are the genetic quirks that shape traits irrelevant to health, such as future height or eye color. In a recent survey, the majority of over 1,000 obstetricians/gynecologists expressed concern about ordering genetic tests that could reveal nonmedical traits. These doctors also wondered if genetic information overload would boost parents’ anxiety, leading to unnecessary and costly treatments, researchers reported in 2016 in Prenatal Diagnosis.
That’s not to say whole-genome tests should never be used. The tests should be considered when doctors suspect a genetic abnormality that hasn’t been uncovered by other methods, the position paper notes. When this happens, it’s best to also look at the parents’ genomes to get a clearer picture of the genetic trouble. These tests ought to always come with lots of discussions between health care providers and parents, before and after testing.
A two-faced star just helped weigh an extra-massive pulsar.
The star takes about four hours to orbit its companion, a fast-spinning stellar corpse called a pulsar that’s about 10,000 light-years from Earth. That means the pair’s orbital dance is tight enough that the star always shows the same face to the pulsar, similar to how the moon is oriented to Earth.
Radiation from the pulsar has fried the near side of the companion star to a scorching 7800° Celsius, Manuel Linares of the Polytechnic University of Catalonia in Barcelona and colleagues report May 23 in the Astrophysical Journal. That’s as hot as an A-type star, which are typically around twice the mass of the sun and burn at higher temperatures. But the side facing away from the pulsar is just roughly 5400° Celsius, similar to stars like the sun. Linares and colleagues also measured the Doppler shift — the change in the wavelength of the star’s light as it moves toward and away from the Earth — of the star’s two sides as it moved around the pulsar to calculate its orbit precisely. The team used that precision to estimate the mass of the pulsar, and found it was surprisingly heavy: around 2.3 times the mass of the sun.
A type of neutron star, pulsars are extremely dense, cramming the mass of a star into an orb the size of a planet. Previous studies of packing neutrons together at high pressures had suggested that a pulsar can’t be more massive than 2.2 solar masses without collapsing into a black hole (SN: 12/23/17, p. 7). The new finding may force a rethink of how these particles interact at high densities, Linares says.
The duo, named PSR J2215+5135, is called a “redback” binary, after the cannibalistic spider of the same name, because the pulsar is gradually stealing material from its neighbor. Eventually, the pulsar may gobble enough of the regular star to become a black hole. But at the rate the pulsar is eating, this pair seems to be stable. “They will keep dancing for a while,” Linares says.
Police are using a new type of DNA sleuthing, called genetic genealogy. Already the technique has caught murder and rape suspects in California and Washington. While solving the cases has given cause for celebration, the tactics used in catching the alleged culprits have many privacy and civil rights experts worried.
Closing the Golden State Killer case (SN Online: 4/29/18) and the previously unsolved double murder of a young Canadian couple (SN Online: 5/23/18) involved probing a public online database of people’s DNA and family-tree information called GEDmatch. In a May 29 opinion piece published in the Annals of Internal Medicine, bioethicist Christine Grady and colleagues argue that police should be more transparent about how they use forensic DNA searches. Meanwhile, law professor Natalie Ram and colleagues go even further in an essay in the June 8 Science, writing that eroding limits on the use of crime-solving technology “threatens our collective civil liberties and opens the door to socially and politically unacceptable genetic surveillance.”
Here are a few key points in the debate:
Why are police using GEDmatch instead of DNA testing companies? If police wanted to use 23andMe or AncestryDNA to help solve crimes, they would need a clean saliva sample from a potential suspect to send to the company for testing and analysis. But crime scene DNA doesn’t come in that form, so police can’t send DNA to the companies for testing. That’s not the case with the DNA analysis service GEDmatch, to which customers can upload raw DNA data received from testing companies.
“That means the police or law enforcement investigators are equally able, if they have enough DNA to create a sufficiently complete genetic sequence, to upload that to GEDmatch” to find potential suspects, says Ram, of the University of Baltimore School of Law.
Companies like 23andMe and Ancestry also require consent from the person the DNA belongs to before the companies will do testing. That’s, obviously, not possible with crime scene DNA. However, GEDmatch in May changed its terms of service “to explicitly embrace the use of their service by law enforcement,” Ram says.
Could these searches lead to people being investigated needlessly? Before police tracked the Golden State Killer suspect through GEDmatch, investigators subpoenaed Family Tree DNA for information about a customer whose Y chromosome partially matched DNA from one of the crime scenes. Police then used that information to order a man in an Oregon nursing home to give a DNA sample. He was not a match.
“Just having DNA match something at the crime scene doesn’t mean the person committed the crime,” says Grady, who heads the National Institutes of Health Clinical Center’s Department of Bioethics in Bethesda, Md. “It just means that they were there, or something that they used was there.” Police still have to prove the suspect committed the crime.
If DNA tests are helping to catch criminals, shouldn’t we be all for it? “Catching criminals is great,” Ram says. “But privacy is also important. Police could solve more crime if they, for instance, could go rifle through anybody’s home at any time for no reason.” But such searches are illegal, because they violate people’s rights to privacy and security against unreasonable search and seizure.
Some people have suggested this type of search could be limited to solving very serious crimes and cold cases. But such limits have been tried before, Ram notes. Over the past decade, some U.S. states have begun allowing the use of police DNA databases for “familial searches.” Such searches may implicate close relatives of people in the police database as suspects in a crime. “States that embraced that technology initially said, ‘we’re only going to use this for really, really serious crimes.’ ” But then Colorado in 2009 convicted its first suspect with this technique — for “a burglary where someone broke into a car and stole about a dollar and a half in change,” Ram says.
Many people say DNA data should be treated differently than other personal information. “There are things that are unique about genetic data. Most importantly, that it has implications for others,” Grady says. People strive to protect medical information, but medical records reveal things about only an individual. DNA reveals things about relatives, too.
“If I give up my genetic data, you can learn things about people who are related to me that you can’t learn from my cholesterol or my blood pressure, or even my psych history,” Grady says. There should be some safeguards, she adds. “No law enforcement agencies have rules or standards about how they use this kind of information.”
Do any laws protect against this type of search? Because GEDmatch is a public database, privacy protections that govern private companies probably don’t apply. “If people voluntarily put their data on GEDmatch, they’ve given it away,” Grady says. It’s like they’ve cut their hair and left the hair on the floor. There’s no protection for that.” Other laws governing the privacy of genetic and medical information don’t apply genealogical DNA data deposited in public databases.
But Grady believes that could soon change. “I suspect there will be people entertaining new laws in light of the recent uses.”
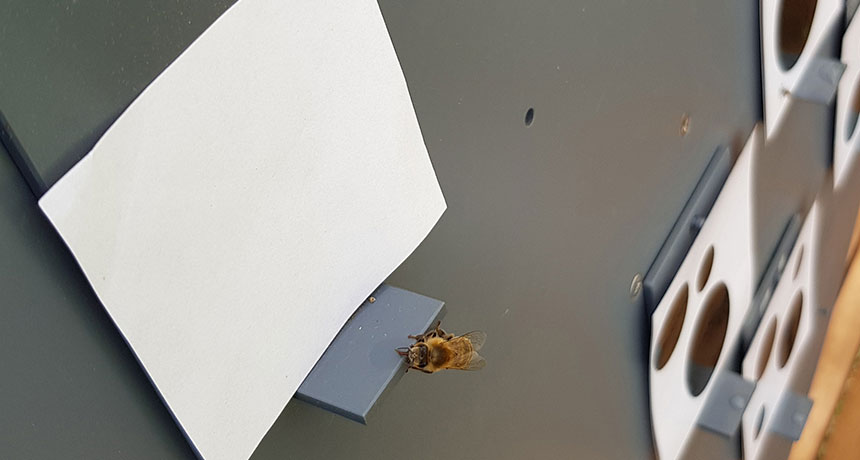
A little brain can be surprisingly good at nothing. Honeybees are the first invertebrates to pass a test of recognizing where zero goes in numerical order, a new study finds.
Even small children struggle with recognizing “nothing” as being less than one, says cognitive behavioral scientist Scarlett Howard of the Royal Melbourne Institute of Technology in Australia. But honeybees trained to fly to images of greater or fewer dots or whazzits tended to rank a blank image as less than one, Howard and colleagues report in the June 8 Science. Despite decades of discoveries, nonhuman animals still don’t get due credit outside specialist circles for intelligence, laments Lars Chittka of Queen Mary University of London, who has explored various mental capacities of bees. For the world at large, he emphasizes that the abilities described in the new paper are “remarkable.”
Researchers recognize several levels of complexity in grasping zero. Most animals, or maybe all, can understand the simplest level — just recognizing that the absence of something differs from its presence, Howard says. Grasping the notion that absence could fit into a sequence of quantities, though, seems harder. Previously, only some primates such as chimps and vervet monkeys, plus an African gray parrot named Alex, have demonstrated this level of understanding of the concept of zero (SN: 12/10/16, p. 22).
The researchers first trained bees to visit a spot with either a Y-shaped maze or an upright display, both offering images with different numbers of elements, such as dark circles of different sizes. Some bees were trained to fly to the image with the lower numbers of objects, while other bees were taught to go to the higher-number image. The researchers offered the bees a sweet treat for the correct image, and a bitter quinine solution for a wrong answer.
“I was fairly afraid of bees when I began working with them,” Howard says. But learning their ways convinced her that a lot of what humans mistake for aggression from a foraging bee buzzing around is usually “just curiosity.” The trained bees then performed a series of tests with no rewards. In one test that offered the bees a choice between a single shape image versus a blank image, bees trained to pick the lower number of objects flew to the blank image — the zero — 63 percent of time. Overall, the test results showed the bees treating zero as being less than one, Howard says.
The results convince evolutionary behavioral biologist Rafael Rodríguez of the University of Wisconsin–Milwaukee that honeybees are indeed getting the basics of zero. Now he’s wondering about earlier studies that might hint that certain spiders would be worth testing, too.
Still, the most sophisticated sense of zero, using a symbol for it in mathematical calculation, is a feat only humans have demonstrated. So far. Howard muses about the possibility of someday testing bees’ prowess on that harder feat.
I’m making my way through my third round of breastfeeding a newborn and taking stock of how things are going. Some aspects are definitely easier: My milk came in really quickly (a perk of being a repeat lactator), the fancy breastfeeding baby holds are no longer mysterious to me and I already own all of the weird pillows I need to prop up my tiny baby.
But one thing isn’t easier this time around: the bone-crushing, mind-numbing exhaustion. Just like my other two, this sweet baby seems to eat all the time. All day. All night. Sometimes multiple times an hour, especially in the witching hours of the evening. This frequency got me curious about the biology of newborns’ stomachs. Just how small are they? Are they so microscopic that one can hold only enough sustenance to keep my newborn satisfied for a thousandth of a second? Birth educators and medical professionals often use a marble to illustrate the size of a newborn’s stomach, a tiny orb that holds about 5 to 7 milliliters of liquid. But that small estimate has come into question. A 2008 review published in the Journal of Human Lactation points out that there aren’t many solid studies on the size of the infant stomach, and some of the ones that do exist come to different conclusions. Another review of existing studies concluded that the average newborn stomach is slightly smaller than a Ping-Pong ball and can hold about 20 milliliters, or about two-thirds of an ounce.
The question of stomach size at birth isn’t settled, and that may be in part because there is no one answer. Just as babies come in a variety of sizes, their stomachs may too. What’s more, size isn’t everything. Drinking ability, the stretchiness of the stomach and the speed at which food gets digested are all part of the equation, and those physiological skills may take a few days, or longer, to get sorted out. There’s evidence that brand new stomachs get better at relaxing after a few days, which lets them expand and hold more liquid, for instance.
Because we don’t really know how big any particular newborn’s stomach is, the best approach to feeding frequency comes from watching the baby’s behavior. Babies should be fed on demand, the American Academy of Pediatrics recommends. And babies “demand” a meal — either breastmilk or formula — by rooting around with their heads or starting to suck on something (their hands, their parents’ arms, whatever’s within reach). Crying is often one of the last signals they send. Breastfeeding sessions should be attempted eight to 12 times in a 24-hour period.
We’re definitely in round-the-clock territory in my house. During a recent back-to-back nursing session, I had a vague memory of a study on the !Kung hunter-gatherers of Namibia and Botswana. Reading the study again gave me a whole new appreciation for these women. During the daytime (when researchers were observing), the women’s babies, who ranged in age from 12 weeks to more than 2 1/2 years, nursed an average of four times an hour, with about 13 minutes between nursing bouts. Those astonishing numbers put my own nursing marathons into perspective, and reminded me that the struggle to keep up with growing babies’ appetites is universal.
As the Hawaiian volcano’s latest outburst enters its third month, scientists are still watching Kilauea 24/7. Such constant monitoring not only provides danger warnings aimed at keeping those nearby safe, but it also offers remote viewers the rare opportunity to observe the evolution of an eruption in real time.
As magma within Kilauea’s summit crater, called Halemaumau, continues to drain and move toward the lower east rift zone, the crater floor is becoming increasingly unstable. The U.S. Geological Survey has observed frequent rockfalls into the crater since mid-May; each collapse triggers a small explosion. One of the largest explosions happened June 30, when a collapse-explosion cycle released energy equivalent to a magnitude 5.3 earthquake. While a “Whomp!” and a slow-rising cloud of volcanic gas and ash marked that collapse, the real pyrotechnics are happening along nearly two dozen fissures, vents through which lava erupts, in that lower east rift zone. Lava fountains spurting from two fissures, Nos. 8 and 22, are feeding most of the lava flows now pouring into the ocean.
It’s hard not to stare slack-jawed at images of molten rock spurting into the air, of glowing, fast-moving rivers of lava rushing into the ocean, or of the tangles of wispy-sharp shards of glass known as Pele’s hair. Check out these highlights of Kilauea’s show and the science (and volcanic vocabulary) we’re learning from them. Of nearly two dozen fissures, No. 8 at the eastern edge of the now devastated Leilani Estates neighborhood is producing some of the most spectacular pyrotechnics, including this lava whirlwind, or lavanado. Lavanadoes form much like “firenadoes” do from the wrath of wildfires: Intense heat (in this case, from the volcano itself) causes air to swiftly rise and form a tall column, and strong winds can then cause the column to rotate. Here, the lavanado dances with the molten rock before flinging the lava several meters away. In the vog A thick fog curls out of fissures and seeps along the ground. Dubbed vog, this volcanic smog forms as sulfur dioxide and other gases and particles seeping out from the fissures react with oxygen, water vapor and sunlight. Since Kilauea began erupting along its lower east rift zone, within Leilani Estates, scientists warned anyone in the vicinity to wear protective masks due to emissions of this toxic air pollution. Ropy rock The kind of lava erupting from Hawaiian volcanoes, a molten basalt rock, cools into two main types of formation. When the lava flows slowly, air cools its “skin”— but beneath that skin, the lava continues to ooze ahead, advancing toe by toe. The smooth, ropy skin and toe-shaped lobes are characteristic of pahoehoe lava. By contrast, more swiftly flowing lava, known as Aa, appears chunky and angular. That’s because faster-moving lava loses heat more quickly and becomes more resistant to flow. Instead of a slow, sinuous advance, the lava tears ahead, forming large, hardened chunks.
Fast flow Glowing torrents of lava fed by fissure 8 on Kilauea’s lower east rift zone jet through a channel at speeds of about 7.7 meters per second. USGS scientists shot this video June 19, but the rivers continue to flow. Much like a river of water, flow is fastest at the center of the river and slowest along the edges of the lava channel due to friction. Lava waves form as the molten rock sloshes through lava rapids, along its 13-kilometer journey before it spills into the ocean.
On a boat Also like many water rivers, the lava rivers have occasional passengers. Lava boats are rafts made of pieces of hardened lava that clump together and get carried downstream, like boats on a waterway. A huge chunk of lava, dubbed a lava boat, sails away on this river of lava as Kilauea erupts.
As the lava boats travel, more pieces of lava may cool and glom onto their surface, forming accretions called lava balls.
Toxic steam As Kilauea’s rivers of fire pour into the ocean, they boil the water, sending great clouds of corrosive steam billowing into the air. The steam is a concoction that volcanologists call laze, or lava haze, and it’s the product of a chemical reaction between the hot lava and seawater. The lava, at a temperature of about 1150° Celsius, basically boils away the seawater, leaving behind very reactive sea salts, such as magnesium chloride. These salts react with the steam to form hydrochloric acid. Similar in strength to weak battery acid, laze can irritate eyes and skin, and cause breathing difficulties.
Glass hair When tiny droplets of lava spray into the air and rapidly cool, they can form fine threads of volcanic glass. Dubbed Pele’s hair, they are named for the Hawaiian goddess of fire and volcanoes. The fibers are so fine that they can be carried along by the wind before raining out. But it’s not a gentle rain: The sharp threads are abrasive enough to scratch car windshields and can irritate skin and eyes, or contaminate open water reservoirs.
The new lava delta filling in what was once Kapoho Bay now spans more than 162 hectares, USGS scientists say, the equivalent of more than 300 U.S. football fields. And with the eruption – and Kilauea’s pyrotechnics – showing no signs of slowing (SN Online: 5/8/18), the Big Island will probably continue to grow.
When President Donald Trump took a mental test as part of his physical in January, the results called attention to far more than his fitness for office. (He passed with a perfect score, according to his physician.) It put a test commonly used to catch early signs of dementia in the spotlight. That publicity could lead to missed diagnoses, researchers warn July 16 in JAMA Neurology.
Google searches of the Montreal Cognitive Assessment, a 10-minute screening test consisting of 30 questions, spiked in the week after news coverage of Trump’s physical. Of 190 news articles about his performance identified by the researchers, 53.7 percent included some or all of the test’s questions and answers. And 17 percent encouraged readers to see how their mental abilities stacked up against the president’s.
That might make it more difficult for clinicians to screen patients for early signs of dementia. Taking the test once increases your score the next time you take it, a phenomenon called a learning effect. The study didn’t track how many readers took the memory test. But for those who did, researchers say, the learning effect could artificially inflate some patients’ scores and make it harder for doctors to pick up on the memory symptoms linked to Alzheimer’s and other neurodegenerative diseases.
Most of the news articles quoted questions from one specific version of the test, so the researchers suggest that doctors should administer alternate versions to prevent skewed results.